Clinical Documentation: A Critical Skill for Healthcare Professionals
May 3, 2021
5 min. read

Communication works for those who work at it. John Powell
Clinical documentation is a critical skill for healthcare professionals. Within a healthcare organization, the quality of professional writing reflects the clinicians abilities, department within an organization, and their health profession. Like any skill, professional writing can improve with practice.
Several strategies are available to simplify the writing process. The following approaches to clinical documentation can be modified for any practice setting or health profession.
Writing Functional Problem Statements
During the initial evaluation, a clinician identifies top problems resulting from the clients condition. Treatment goals are derived from this list of identified problems.
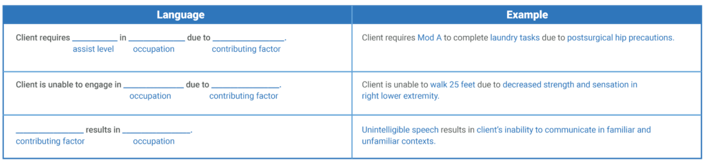
Writing functional problem statements facilitates the development of measurable treatment goals. According to Gateley and Borcherding, functional problem statements consist of two parts:1
An occupation or activity of concern, such as activities of daily living, education, or work
A contributing factor, such as a deficit addressed in treatment, motor and process skills, or body structures and functions
Gateley and Borcherding also provide the following templates to assist in writing functional problem statements:
Writing Measurable Treatment Goals
Treatment goals articulate what the client hopes to accomplish by the time of discharge. In most cases, the clients top problems are used to develop long-term treatment goals.
SMART Goals
Several existing strategies utilize acronyms to make goal writing easier. The SMART method2 is a popular goal writing strategy used across practice settings and health professions.
SMART goals are:
SpecificDescribe what the client will do.
MeasurableDescribe how you will know the goal has been met.
AttainableDescribe what is realistic and achievable considering the clients strengths and availability of resources.
RelevantDescribe what is important to the client.
Time-BasedIndicate a reasonable time frame when the goal needs to be completed.
Example:Client will imitate five signs to make requests with familiar listeners and minimal prompting 80 percent of opportunities for 4 out of 5 consecutive sessions by 5/15/21.
The Coast Method
The COAST method, developed by Crepau, Boyt Schell, and Cohn,3 is another approach that simplifies goal writing.
Measurable goals under the COAST method include the following elements:
ClientDescribe what the client will do using an action verb.
OccupationList the occupation, task or activity that pertains to the problem statement.
Assist LevelSpecify the level of assistance, or level of independence expected.
Specific ConditionSpecify any other conditions under which the client will perform, such as location, compensatory strategy, or use of adaptive equipment.
TimelineIndicate the timeframe by which the goal is expected to be accomplished.
Example:Client will perform a three-step cooking process with two verbal cues from wheelchair level by 5/15/21.
SOAP Notes
The SOAP note is one of the most widely adopted approaches to clinical documentation used by healthcare professionals.4
The acronym SOAP provides an outline to organize information based on the main features of a treatment session. Gateley and Borcherding suggest using the following SOAP note format:
Subjective:
Provide a brief subjective statement that reflects something significant the client (or caregiver) shared about his or her condition or treatment.
Include a direct quote or brief summary of what was said.
Objective:
Describe the length, setting, and purpose (i.e., targeted deficits) of treatment.
Include measurable and observable data related to treatment goals and objectives.
Use action verbs to indicate active participation by the client and clinician.
Be specific about levels of assist provided and use of standard abbreviations.
Assessment:
Analyze and interpret the events reported in the subjective and objective sections.
Note the clients progress, problems, and rehabilitation potential.
Justify continuation of services by indicating what the client still needs to work on.
Plan:
Describe what will happen next. Include the frequency and duration (for example, two times per week for four weeks), purpose of future sessions, and specific intervention strategies to be used.
Specify recommendations and/or referrals to outside services and agencies.

Guidelines for Clinical Documentation
Be concise.
Use people-first language.
Correct errors in spelling, grammar, and punctuation.
Use appropriate terminology.
Only use abbreviations and symbols that have been approved by your facility.
Remember If it was not documented, it never happened.
5 Assumptions for Clinical Documentation
Clinical documentation serves many purposes. This technical style of writing provides a tool for communication, as well as financial and legal accountability for the healthcare organization.
Gateley and Borcherding propose several assumptions to keep in mind before submitting clinical documentation to a clients permanent health record:
Other members of the healthcare team need to read and understand what I write to coordinate care within and between practice settings.
My writing will be scrutinized by third-party payers such as Medicare, Medicaid, and private insurance companies to determine if the services provided justify reimbursement.
My clients health record is a legal document. My writing must be clear, accurate, and thorough should I ever be called to testify in court.
What I write in my clients health record may be utilized for education and research purposes by students and public health entities.
My clients will exercise their right to read their health record.
Keep your documentation skills fresh and with Medbridges library of courses, including:
Documentation: Reporting Skill and Progress (series)
Identifying, Communicating, and Documenting Patient Change in Condition
Below, watch Diana (Dee) Kornetti discuss setting SMART goals for patients in a short clip from her and Cindy Krafft's MedBridge course, "Defensible Documentation in Home Health: Care Planning & Goal Setting."

Meet the Author


Subscribe to Our Newsletter
Related Posts

January 4, 2022
What Makes Documentation Defensible?
By Ellen Strunk

March 20, 2025
Home Health Documentation Template: A Guide to Clear, Compliant, and Consistent Records
By Tina Marrelli

August 8, 2017
9 Secrets to Successful Patient Engagement
By Todd Davenport

July 5, 2020
13 Questions to Ask When Evaluating a Complex Elbow Injury
By Jennifer T. Dodson