Adapting Manual Therapy to Telehealth and Virtual Care
July 6, 2023
5 min. read

Technology use in healthcare sometimes feels like a perplexing dichotomy. For example, new surgical techniques, imaging modalities, and medications are constantly being developed. However, the user interface of some electronic medical records and the reliance on age-old communication methods, such as faxes, feels stuck in the past.
Regardless, as technology improves and access to HIPAA-compliant video chat software becomes more available, the age of telehealth is upon us. Those who desire or require the convenience of staying at home are now more easily able to continue accessing healthcare needs like primary care, specialist care, or allied health like rehabilitation services. This is extremely important for those who are medically fragile or who live in remote regions where the nearest medical center could be hours away by car.
Spurred on by the advent of the COVID-19 pandemic, telemedicine is on the rise, and allied healthcare and rehabilitation professionals must be ready to adapt to its advantages and challenges.
Pros and Cons
A unique advantage of telehealth for allied health and rehabilitation professionals is that we are able to work with the patient in their home environment. From working on body mechanics during ADLs to ergonomics at a desk or workstation and fall risk assessments of the environment, there are a multitude of ways that outpatient services can now help with in-home situations.
Conversely, there are also challenges to adapting to telehealth as rehabilitation professionals specifically, regarding manual therapy. There are many things that we do to stretch, mobilize, assist, and cue our patients with hands-on methods. These must be re-evaluated, and analogues must be found for virtual healthcare. Hands-on techniques, like joint mobilization and soft tissue mobilization, can prove particularly challenging.
What Are Our Options?
If our aim is to provide improved muscle flexibility and joint mobility to our patients without the use of hands-on mobilizations, there are a few options:
Self-stretching: First, we can simply let the patient stretch to improve their joints range of motion as they normally would in a home exercise program. This has the advantage of being quite easy to teach; however, it may not address restrictions in the targeted way a mobilization would. The biggest advantage with stretching is that it is something most clinicians are familiar with teaching to their patients, so the transition to telehealth is not as challenging. Take a look at the video below of a therapist teaching a stretch to their patient in a virtual visit.
Self-soft tissue mobilization: Clinically, soft tissue mobilization is often paired with stretching to attempt to improve effectiveness. In trying to reproduce this at home, usually some piece of equipment is helpful. For example, if a patient has a foam roller, that can be a very useful self-soft tissue mobilization tool. However, if they do not, a rolling pin used for baking or even a stainless-steel water bottle is a potential replacement! You can see an image below of a therapist teaching her patient to mobilize her peroneal muscles with a rolling pin. A small disadvantage of this type of self-mobilization is the patient must have enough flexibility elsewhere in their body to reach the area in question. If not, there are certainly other ways they could self-mobilize their peroneal muscles. It would simply require a little more creativity!

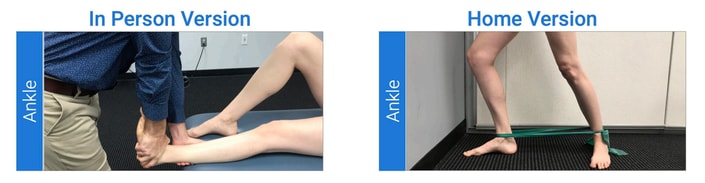
Self-joint mobilization: What if the patients muscles are not the limiting factor? Our next option is to try to find a way to reproduce joint mobilization at home. This has the advantage of being the targeted type of joint capsule stretch the patient needs but can be more challenging to teach to the patient and may require some equipment to set it up. Below, you can see an example of two different ankle dorsiflexion self-joint mobilizations using an exercise band. The band provides the posterior glide to the talus and the patient performs a mobilization with movement into dorsiflexion passively, using her back foot to guide the movement.
Partner-assisted mobilization: Our final option is to recruit the help of a spouse, caregiver, or other family member to help provide the mobilization. This has the advantage of keeping the patients body in a more passive, less active, position which can help with reducing muscle guarding. However, it requires significant education to the family member, and care must be taken based on the patients irritability and symptom response. It would be best to have the patient and assistant perform these during a telehealth session, so that the patients response could be measured, and you can make sure the desired outcomes are occurring, such as less pain and more ROM. If the patient and family member both agree and are capable, you can teach them to perform cervical or hip joint distraction with relative ease as shown below.

Whats Next?
My Medbridge course Telehealth: Delivering Virtual Interventions has a series of self-joint mobilizations for commonly affected joints to start you off, but we are only limited by our creativity! Imaginative use of bands, ankle weights, and nearby helpers creates a wide array of options that we can tailor fit to each individual patients needs. Telehealth need not be the end of manual therapy, but the expansion of different ways to promote the patients self-efficacy in their own treatment.
Below, watch Jared Vagy discuss home equipment suggestions during a telehealth visit in this brief clip from his Medbridge course, “Telehealth: Delivering Virtual Interventions."
Meet the Authors


Subscribe to Our Newsletter
Related Posts

April 5, 2022
The Value of Pediatric PT and Telehealth: More Than Our Hands
By Sierra Christensen

October 14, 2020
The Future of Healthcare: Integrating Telehealth in the Care Continuum
By Jared Vagy

April 16, 2020
Incorporating Telehealth into Home Health Care Part 1: Practical Strategies
By Ellen Strunk, Kara Gainer, and Kenneth L. Miller

December 21, 2023
Solve for Access, Engagement and Outcomes with Virtual Care Delivery
By Medbridge