Translations of the Scapula
Whether you’re rehabbing an elite athlete, weekend warrior, or a person with a total shoulder replacement, getting a better grip on all the complex movements of the scapula, as well as what is and isn’t normal, provides much-needed context for better exercise prescription and patient education.
August 18, 2021
3 min. read

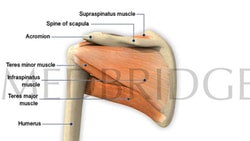
In previous articles, we've looked at the scapula's complex anatomy, which allows it to move as freely as it does and play such a crucial role in human function, as well as the scapula's rotations.
This time, we're going to take a closer look at the variety of translations of the scapula and how those work. Understanding all of these complex motions of this joint provides you with the deep insight you need when rehabilitating a person with a scapular injury so they can return to sport.
Lateral Translations and Medial Translations
Two translations can occur in the presence of an intact clavicular strut and acromioclavicular joint. These are:
Upward and downward sliding on the thorax due to clavicular upward and downward motion at the sternoclavicular (SC) joint
Anterior and posterior sliding around the curvature of the thorax due to clavicular anterior and posterior motion at the SC joint
You have likely been taught that anterior and posterior sliding is called protraction and retraction. This is not entirely accurate.
First, since these actions are performed voluntarily (to some extent), the translations can be viewed as physiologic motions. Second, since a translation is technically a joint play motion described as a "slide," then protraction and retraction do not accurately describe that action.
Instead, when the scapula is sliding laterally and anteriorly, it is more accurate to call the action "lateral translation," and the term "protraction" should describe the end position once the scapula has moved as far anteriorly as it can. In other words, a person must laterally translate the scapula in order to achieve an end position of protraction. Conversely, a person must medially translate the scapula in order to achieve an end position of retraction.

Considering Muscle Fiber Orientation
While the translations are relatively straightforward, one point you should consider—as we did in our discussion about rotations—is muscle fiber orientation. For example, let's look at elevation and depression. You might assume that elevation and depression occur linearly, sliding vertically up or down the thorax. As with protraction and retraction, this isn't quite accurate.
The three muscles responsible for elevation, the upper trapezius, the levator scapulae, and the rhomboids, are all oriented in an angular fashion. This suggests that "normal" elevation is not perfectly vertical but instead diagonal toward the cervical spine and head.
This is important to understand because:
When you see someone "shrug" on clinical examination and the scapula moves vertically rather than diagonally, you know there is a muscle or nerve issue that needs to be addressed.
Patients should not be taught to perform rehabilitation exercises involving scapular elevation that is perfectly vertical.
This same phenomenon occurs with depression. Muscle orientation of the lower trapezius and latissimus dorsi suggests that true depression contains an inferior medial diagonal component. Another key feature about scapular depression is that it is common to see variations in concomitant motion between individuals. The scapula can remain in a neutral position during depression, but it is possible to see lateral translation or medial translation as a normal variant.1
Whether you're rehabbing an elite athlete, weekend warrior, or a person with a total shoulder replacement, getting a better grip on all the complex movements of the scapula, as well as what is and isn't normal, provides much-needed context for better exercise prescription and patient education.
Below, watch Jared Vagy discuss quantifying and addressing scapular winging in a short clip from his MedBridge course, "The Movement System: Scapular Syndromes of the Shoulder."
Meet the Author


Subscribe to Our Newsletter
Related Posts

July 30, 2019
The Role of the Scapula
By Aaron Sciascia

November 21, 2019
From Dancing to Dunking: Rotations of the Scapula
By Aaron Sciascia

January 12, 2023
Defining Scapular Dyskinesis and Its Causes
By Aaron Sciascia
March 30, 2016
Shoulder Biomechanics and Exercises
By Robert Donatelli